

Diabetes (diabetes mellitus) is a common disease in which blood-sugar levels are chronically too high. The disease has many related complications and several eye diseases are among them. The most common eye complication of diabetes is diabetic retinopathy, a leading cause of adult blindness.
Background
The retina is a thin, light-sensing layer in the back of the eye. If the eye is thought of as a camera, the retina can be equated to the film of a camera. The importance of this layer cannot be over-emphasized. Just like in a camera, even with the perfect lens in place, the eye can’t see clearly without healthy, regular ‘film’ (retina). Light rays are focused by the cornea and natural lens (the ‘camera lenses’ in our analogy) onto the retina, where they are perceived and then transmitted to the brain. At the center of the retina is the macula, a very small but very precise area of the retina that is responsible for the majority of our fine, precise vision. It is this part of the retina that helps us to see and recognize faces, read letters in print, and to drive, etc.
Diabetes is the leading cause of blindness for people between 20-64 years old. It accounts for 12% of all new cases of blindness in the United States!
Any disturbance of the vessels or architecture of this very precise layer of the eye can cause loss of vision, distortion of images or shapes, or even blindness. Diabetes can cause such changes and is the leading cause of blindness for people aged 20-64 years.
What is Diabetic Retinopathy?
Diabetic retinopathy is a common but potentially blinding eye condition in which the vessels in the back of the eye change and become dysfunctional.
In the early phases of the disease, the small vessels of the eye (the capillaries) will leak fluid or blood. This can lead to swelling of the retina or the macula, which may result in blurring or distortion of central vision. This is especially true when the center of vision gets swollen (called Macular Edema).
As the disease progresses, the vessels can bleed into the retina or into the vitreous, the middle, normally fluid-filled part of the eye that is usually transparent (read more here). This can cause spots, or floaters, in the central vision and may block almost all of the light from arriving at the retina and thereby being perceived.
Finally, in its more severe stages, diabetic retinopathy can cause occlusion of vessels and thereby cause proliferation of new vessels. When the vessels of the eye get occluded, this can lead to macular ischemia where the central macula is deprived of the blood and oxygen it needs to function properly. This leads to blurred vision and potentially permanent visual loss. Moreover, this prompts the body to form new vessels. However, these new vessels (the process being called neovascularization) are abnormal and weak, and they tend to bleed and tug on other nearby parts of the retina. If left untreated, this can lead to retina tears, retina detachments, scarring, and eventually loss of vision in the eye.
Who is at Risk for Diabetic Retinopathy?
All people with diabetes are at risk. However, those at higher risks are diabetics with chronically out of control blood sugars. About 40% of Americans with diabetes have some stage of diabetic retinopathy, and within 20 years the majority of patients with diabetes will have some retinopathy. Other risk factors include:
- Uncontrolled blood sugars with high representative A1c’s
- Uncontrolled blood pressure
- High cholesterol/triglycerides (fats in your blood)
- African American, Latino, and Native American Race
- Pregnancy, where diabetic retinopathy can become exacerbated
Signs of Diabetic Retinopathy
Early diabetic retinopathy may have no signs such that the condition goes undiagnosed for years. It is often at this critical time that a timely intervention can prevent further worsening of the disease and loss of vision. However, if left unchecked, the disease may progress into a more serious and less treatable form. This is why it is important to be checked regularly by your ophthalmologist. Early symptoms (once they manifest) can include:
- Spots, dots, or dark strings in your vision (floaters)
- Blurred vision
- Fluctuating vision especially when the blood glucose runs high
- Vision loss
- Color desaturation/washout
- Black or blank spots in vision
- Pain from high pressure in eye
- Sudden loss of vision from a vitreous hemorrhage

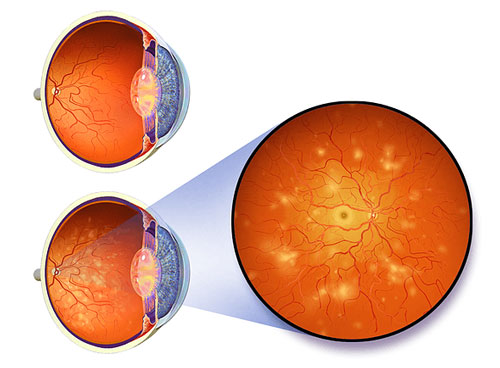
Normal view compared to view with significant diabetic retinopathy “National Eye Institute, National Institutes of Health” The condition can typically be diagnosed by an ophthalmologist during an eye exam, long before noticeable vision symptoms occur and when more treatment options are still available. Thus, it is very important for those suffering from diabetes to have regular eye exams, to monitor for diabetic retinopathy, and other complications. In a typical exam, your ophthalmologist will check your vision, examine your eye in a slit lamp biomicroscope, and check your retina with special instruments. He or she may need additional tests to determine why your vision is blurred, and to help guide treatment. Such tests can include: fluorescein angiogram (FA), optical coherence tomography (OCT); ultrasound (B-scan).
When Should I Be Checked?
You should adhere to the recommended guidelines as to when to first be seen and how you should be followed:
- Type 1 Diabetes: Within 5 years of being diagnosed, then every year thereafter
- Type 2 Diabetes: When diagnosed, then every year thereafter
- During pregnancy: During the first trimester
Your ophthalmologist may need to see you more frequently based on the severity of your disease or the concern for possible progression.
How Can It Be Treated?
Treatments for diabetic retinopathy vary based upon the nature and progression of the condition. The cornerstone of treatment is to vigilantly control blood-sugar levels, lessening the chance of retinopathy, and impeding its rate of advancement. Many studies have shown that strict blood sugar control can slow, stop, or even possibly reverse disease. This is done in conjunction with your primary care physician. Diabetic Retinopathy does not need to be treated in its initial stages, but it does need to be watched vigilantly. Treatment is indicated when new vessels form, or when the swelling/leaking blood vessels involve the macula. Your doctor will talk to you about treatment options.
Laser surgery – this treatment modality uses focused light to target abnormal blood vessels or oxygen-deprived parts of the retina.
It can be used in two fashions:
- To shrink abnormal blood vessels in the macula in order to prevent further swelling (Focal Laser Therapy, FLT).
- To cause regression of the abnormal new blood vessels (neovascularization) by reducing the amount of ischemic and poorly functioning retina (Pan-Retinal Photocoagulation, PRP).
Injections (intravitreal) – medicines (called Anti-VEGF) can be used to treat Diabetic Retinopathy. They target the chemical mediators which trigger the growth of new blood vessels and also help to reduce swelling of the retina.
Vitrectomy surgery – this surgery involves removing the vitreous jelly from the inner portion of the eye. In doing so Vitrectomy also removes blood from within the vitreous. During the surgery, laser can be applied, and other retinal problems can be addressed.
Your ophthalmologist will talk to you about the best treatment option for you given your particular problem and will help you make the best decision for your eyes in order to try to restore any lost vision.